
How much bone density do you lose in the first five years of menopause?
The answer is faster than most women are told, and the window to act is earlier than most think.
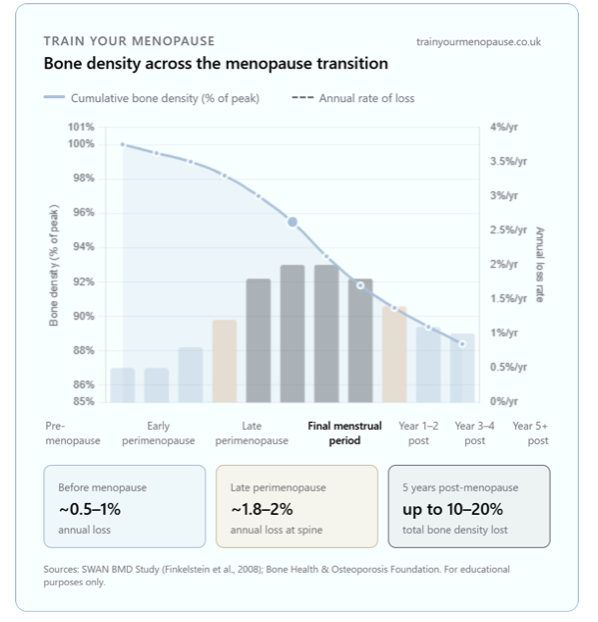
Bone loss isn't something that starts quietly at 60. For many women, it begins around age 35, accelerates at perimenopause, and peaks in the first few years after menopause. More than 1 in 3 women, compared to 1 in 5 men over 50, will sustain an osteoporotic fracture in their lifetime.
Why does this happen so fast?
Bones are constantly remodelling to maintain strength: old bone is removed by osteoclasts (cells that remove bone) and replaced with new bone by osteoblasts (cells that build new bone). Oestrogen is responsible for slowing down the activity of osteoclasts. When oestrogen drops sharply in the menopause transition, osteoclast activity is no longer adequately suppressed, and the balance tips. Bone is broken down faster than it can be rebuilt. If this continues, bones are at risk of developing osteopenia (lower-than-normal bone density) or osteoporosis (significant bone loss), which makes bones more prone to fracture.
What actually makes a difference?
Progressive resistance training is the most direct stimulus for bone formation. The LIFTMOR trial (Watson et al., 2018) demonstrated that high-intensity resistance and impact training produced meaningful improvements in bone mineral density at the hip and spine in postmenopausal women, where lower-intensity exercise had not.
Menopausal Hormone Therapy (MHT) also has robust evidence behind it. When started around the time of menopause, it can prevent the accelerated bone loss 5 years post-menopause. It's worth discussing with your GP or menopause specialist if you haven't already, particularly if you have other risk factors such as low body weight, smoking, a family history of osteoporosis, or an early menopause.
Calcium and vitamin D matter, but they won't build bone on their own. Think of them as the raw materials, the building signal comes from load. Aim for 700–1,200mg calcium daily through food (dairy, leafy greens, tinned fish with bones, fortified plant milks) and check your vitamin D. NHS guidance recommends everyone consider taking 10 micrograms (400 IU) daily in autumn and winter; if you're rarely outdoors, have darker skin, or are over 65, take it year-round.
THE PRACTICAL POINT
Your skeleton remodels in response to mechanical load. Two to three sessions of progressive resistance training per week is the minimum effective dose. Add impact training; jumping, skipping, or brisk walking with a weighted vest, and you cover both the compressive and ground-reaction forces that the bone responds to most.
A DEXA scan gives you a baseline. If you're perimenopausal and you've never had one, it's worth asking your GP whether you're eligible. NICE guidelines (NG23) recommend assessing fracture risk in women presenting with risk factors, and the menopause itself is one of them.
Key references: SWAN BMD Study (Finkelstein et al., 2008, J Clin Endocrinol Metab); Watson et al. (2018), LIFTMOR Trial, British Journal of Sports Medicine; NICE NG23 (2023); Bone Health and Osteoporosis Foundation.
These resources are for educational purposes only and do not constitute medical advice. Please consult your GP, physiotherapist, or menopause specialist before making changes to your exercise, nutrition, or medication.